
Frozen Shoulder | What Treatment is Best?

There is a debate in the literature around which treatment is best for long term management of frozen shoulder surgery, physiotherapy or both.
Frozen shoulder, also known as adhesive capsulitis, is a commonly seen condition in all areas of physiotherapy practice. The condition commonly affects people who are older than 50 years of age and is more likely to occur in people with diabetes, cardiovascular disease, trauma, stroke or neurosurgery.
Diagnosis of adhesive capsulitis is normally based on clinical features of insidious onset pain in the shoulder with increasing stiffness and clinical findings of limited active and passive external rotation without creptius.
Frozen shoulder can spontaneously resolve but up to 40% of patients report persistant symptoms up to and over 4 years after onset. There are a number of treatment options available including manipulation under anaesthetic, where the capsule is torn, and arthroscopic capsular release where the capsule is cut. Physiotherapy instead of or in supplement to surgery is an option for people suffering with frozen shoulder but there is some debate about which treatment works. The UK national physiotherapy guideline for frozen shoulder recommends exercise and manual therapy either in isolation or to supplement intra-articular injection of glucocorticoid (steroid), manipulation, or capsular release.
It is not known whether structured physiotherapy or either MUA or arthroscopic release followed by physiotherapy is more effective. Recent systematic reviews highlighted this gap in understanding and this is why the UK FROST trial was created. To assess the effectiveness and cost-effectiveness of three care pathways to treat adults with a frozen shoulder: two commonly used surgical interventions within the UK National Health Service (NHS) hospitals (manipulation and capsular release), and our specifically designed non-surgical physiotherapy pathway.
Methods
The UK FROST trial is the largest RCT to compare early structured physiotherapy, manipulation under anaesthetic and arthroscopic capsular resease. It was a large multicentre RCT with three parallel groups of patients who were referred to secondary care for treatment of primary frozen shoulder. All patients were randomised via computer algorithm and in a way which reduced the influence of the presence of diabetes.
There were 35 hospital sites involved from across the UK involving 90 surgeons and 285 experiences physiotherapists who were familiar with the treatment protocol used within the trial. This early structured physiotherapy was a multicomponent secondary care physiotherapy intervention, including steroid injection, that we developed using recommendations from national guidelines and a Delphi study of shoulder specialist physiotherapists. The operative group still undertook a post procedural physiotherapy programme which was developed using systematic review, survey and delphi consensus methodology.
Both of the surgical procedures were performed as day cases within 18 weeks of randomisation.
The primary outcome measure used was the Oxford Shoulder Score and the primary end point was 12 months after randomisation. Secondary outcomes included QuickDASH, EuroQOL-5, and VAS score which were all collected at baseline, 3 months, 6 months and 12 months after randomisation.
In total 914 participants took part in the study with 503 randomly assigned to the three treatment groups; 201 MUA, 203 arthroscopy and 99 to physiotherapy. All trial profile and result data are available within the article.
Results and Clinical Importance
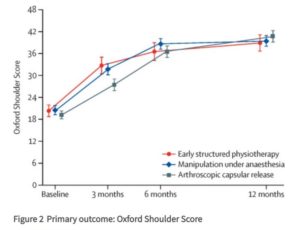
After 12 months the participants who underwent arthroscopic capsular release had the highest OSS score at 40.3 followed by MUA at 38.3 and early structured physiotherapy at 37.2 points. However at 3 months capsular release has the lowest OSS score. A similar pattern in outcome was seen when using QuickDASH. Although these results are statistically significant it is unlikely that they are clincially important. It is thought that a score of 5 on the OSS is clinically significant. As you can see by the graph on the right the outcomes are very closely grouped together at 12 months post randomisation.
Looking at the adverse outcomes of the trial and at the cost analysis arthroscopic capsular release was associated with higher risks and MUA was the most cost effective treatment option.
All three treatment options led to substantial improvements in pain and function and none of the treatments were clearly superior. Perhaps a marginal clinically important benefit of capsular release over physiotherapy could be seen in a bigger population group. The physiotherapy programme could be accessed more quickly than the surgical procedures and is lower in cost but doesn’t offer as much improvement as arthroscopic release however physiotherapy is far safer.







No comments